

Chronic venous leg ulcers (VLU) are commonly seen in general practice. Guest et al (2015) estimate that approximately 1.5% of the adult population in the UK is affected by active leg ulceration, meaning that up to 730 000 patients have open leg ulceration at any given time (Guest et al, 2015). With the implementation of the gold standard treatment – compression therapy – healing rates of 76.3% have been recorded at 24 weeks (O'Meara et al, 2012; Nelson and Adderley, 2016).
Despite improved healing rates, however, recurrence rates are depressingly high. Around 60–70% of all VLUs are reported to recur after healing, with the highest recurrence rate within 3 months and the majority recurring within 12 months (McDaniel et al, 2002; Abbade and Lastória, 2005). A quarter of all patients will experience in excess of 10 episodes of active ulceration in their lifetime (Weller et al, 2013).
Strategies to reduce recurrent venous leg ulcers
Once the VLU has healed, the focus needs to be on the prevention of recurrence. However, despite the high recurrence rate and associated costs of treating open ulceration, current Commissioning for Quality and Innovation (CQUIN) targets for reimbursements emphasise the assessment, diagnosis and treatment of lower leg wounds rather than prevention of VLU recurrence (CQUIN, 2020). The primary prevention strategy is the life-long wearing of compression hosiery (Nelson and Bell-Syer, 2014; Atkin, 2019), which can be facilitated by the health professional; however, rates of patient intolerance are high, and the type/level of compression required to prevent recurrence is currently not clear (Nelson and Bell-Syer, 2014).
One of the most commonly cited reasons as to why patients do not wear compression hosiery is difficulties in applying/removing hosiery (Brown, 2018; Atkin, 2019). Patients are encouraged to apply their hosiery first thing on waking when swelling is reduced; however, many patients have difficulty in applying the hosiery over their toes as they are unable to bend sufficiently, particularly if they are obese (Atkin, 2019). This can be overcome by using application aids or raising the feet on a chair to avoid bending over (Atkin, 2019). Alternate compression strategies, such as using adjustable compression wraps with Velcro-type straps, hosiery systems with zip fastenings or using a lower compression strength, may help with application difficulties (Balcombe et al, 2017; Atkin, 2019).
Unfortunately, studies have shown that many patients do not understand the need to wear life-long compression hosiery post-healing (Raju et al, 2007; Yarwood-Ross and Haigh, 2012; Brown, 2018). The health professional must therefore ensure that the patient understands this by offering information in a format that makes the link between the cause of their venous ulcer, chronic venous disease and how compression therapy will help to manage this. Patients need to be told that although this may not cure them, wearing compression hosiery will help minimise the risk of ulcer recurrence (Atkin, 2019), and this may help to encourage patients to persevere with the application of hosiery. Offering patients a choice of type of hosiery, such as flat knit rather than circular knit, which tends to be more difficult to apply, a lower level of compression strength and a different colour, may also encourage adherence (Tandler, 2016). Although a high level of compression may be clinically indicated, prescribing a lower level may ensure that the patient wears his/her compression hosiery, as any level of compression is better than none at all (National Wound Care Strategy Programme, 2020).
Self-care to prevent recurrence
Current CQUIN targets for reimbursements focus on the assessment, diagnosis and treatment of lower leg wounds rather than on prevention of VLU recurrence (CQUIN, 2020). It is unlikely, therefore, that clinicians in general practice will be able to offer on-going prevention management routinely and may be restricted to a one-off appointment only. There is some post-healing service provision available, such as Lindsay Leg Clubs®, which are run on a social model (Galazka, 2020) and ‘members’ are encouraged to attend post-healing for monitoring for recurrence and social interaction; however, these clubs are not available in all locations. As a result of this, health professionals will need to encourage patients with healed VLUs to perform some self-care activities to prevent their ulcer recurring. Although the key activity is the life-long wearing of compression hosiery, there are other self-care activities that patients should be encouraged to perform.
Physical exercise and mobility
Finlayson et al (2018) suggest that the evidence on poor mobility as a risk factor for recurrence is inconclusive. Barwell et al (2004) found no association between patient mobility and either healing or recurrence. However, others have suggested that patient mobility and/or restricted ankle movement were significantly related to recurrence rates (Brooks et al, 2004; Vowden and Vowden, 2005; Nelson et al, 2006; Sinabulya et al, 2017). O'Brien et al (2014) conducted a randomised controlled trial to test the effectiveness of a self-efficacy based exercise intervention for adults with VLUs. The intervention group receive an individualised programme of calf muscle exercises and walking. The 12-week exercise programme consisted of up to six behavioural coaching and goal setting sessions delivered via telephone supported by written materials, a pedometer and two follow-up booster calls if required. Participants were encouraged to seek social support among their friends, self-monitor their weekly steps and lower limb exercises, and to perform a total of 150 minutes (30 minutes over 5 days per week) of walking. The control group was supported by a generic information sheet that the intervention group also received encouraging lower limb exercises, a pedometer for self-management and phone calls at the same time points as the intervention group.
Bérard et al (2002) found that strenuous physical exercise, such as running, tennis or football was a predictor for first time ulceration, confirming the findings of Boccolon et al (1997). A study by physiotherapists defined physical activity as daily activities that increase metabolism, such as housework, shopping, transport and walking (Roaldsen et al, 2006). The distance and speed required when walking in order to improve venous return is unclear. Furthermore, van Uden et al (2005) suggested that some VLU patients may walk too slowly to benefit from improved venous return, however Heinen et al (2012) suggest that walking for a minimum of 10 minutes five times weekly at a pace with which they are comfortable would be beneficial to VLU patients.
Heel raises and foot exercises
In the literature, weak calf muscle pump function and limited ankle mobility have been linked to VLU; although it is not clear whether VLU is a consequence of this or whether the ulceration leads to poor ankle mobility and reduced muscle function (Abadi et al, 2007). Physiotherapy-led structured exercise programmes consisting of heel raises, flexion, extension and rotation of the ankles, for 1 hour, twice weekly for 3 months and unsupervised for a further 3 months have been found to strengthen calf muscles and joint mobility (Padberg et al, 2004). Other researchers have found that heel raises and ankle exercises improve calf muscle function and venous return, and patients should be encouraged to perform these exercises in order to improve the hemodynamic parameters of the affected limb (Dix et al, 2003). The precise number of repetitions needed to be beneficial is unclear, but this should be guided by the patient's tolerance of the exercises (Padberg et al, 2004; Roaldsen et al, 2006; Heinen et al, 2007; Jull et al, 2009; Shenoy, 2014).
Leg elevation
Elevating the legs above heart level will reduce leg oedema as the blood flows back to the heart under gravity, resulting in improved venous return (Dix et al, 2005). As a result, patients should be encouraged to rest with their limb elevated for either 30 minutes daily or for 3–4 shorter periods during the day (Abadi et al, 2007). The reason for this is that it has been demonstrated that elevating limbs above the heart by 10-30° is beneficial for transcutaneous tissue oxygen, an indicator of skin perfusion (Heinen et al, 2007). What is not conclusive in the literature is whether compression hosiery should or should not be worn when elevating limbs (Finlayson et al, 2009; Brown, 2012). Anecdotally, this may be the reason why leg ulcers of patients admitted to hospital on long periods of bedrest, often show signs of improvement, even with compression therapy removed (Brown, 2012).
Skin care
It is important that patients care for their skin once their ulcer has healed. This is particularly important if they are wearing compression hosiery as the skin may become quite dry. It is also a good opportunity for patients to inspect their legs for any sign that the ulcer may be recurring, and prompt treatment will increase the chance of more rapid healing. Patients should be encouraged to apply a good quality bland emollient, such as 50% w/w liquid paraffin and 50% w/w soft white paraffin at night when they remove their hosiery (Brown, 2016). This should be applied in the direction of the hair growth, avoiding circular or rubbing movements to prevent folliculitis. Applying this at night-time will enable the emollient to be fully absorbed and will not affect the fabric of the compression hosiery.
Assessing patient self-efficacy to perform self-care activities to prevent recurrence
Finlayson et al (2018) asserted that a self-management intervention could have potential significance in improving the management of people with chronic VLUs but only if an individual's level of exercise self-efficacy and self-management capacity could be improved.
Self-efficacy theory (Bandura, 1977) is a widely used behaviour change model which underpins many interventions designed to promote self-care for a variety of health conditions (Brown et al, 2014). By identifying areas of self-care where patients feel they lack confidence, interventions can be put in place to strengthen their self-efficacy beliefs to perform these activities successfully. A VLU-specific tool has been developed to assess patients' self-efficacy in performing recurrence prevention activities. Figure 1 outlines one of the subcategories – general self-care – which has been found to reliably predict which patients are most at risk of recurrence (Stewart, 2019). These findings were also confirmed by Probst et al (2019) and Turcotte et al (2020) who further validated the tool and translated into Swiss French. A copy of the complete English tool can be obtained by emailing abrowne61@aol.com.
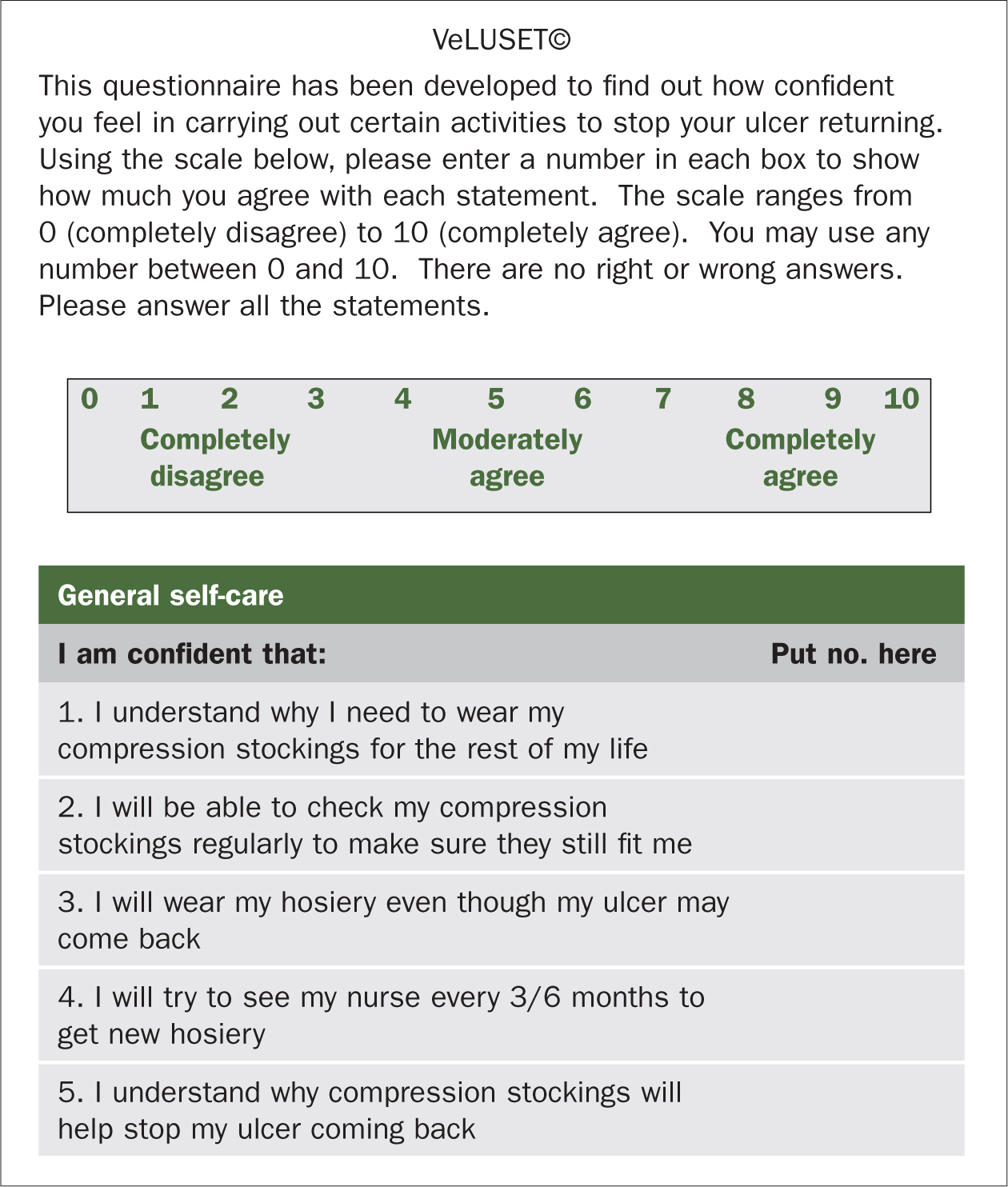 Figure 1. Venous leg ulcer-specific tool to assess self-efficacy in performing general self-care recurrence prevention activities
Figure 1. Venous leg ulcer-specific tool to assess self-efficacy in performing general self-care recurrence prevention activities
A risk assessment tool for recurrent VLUs in the community setting has been developed and validated and found to have good inter-rater reliability in predicting ulcer recurrence (Parker et al, 2017; Finlayson et al, 2018).
The purpose of both these tools is to provide both clinicians and patients with a way of identifying the risk of ulcer recurrence and provide knowledge on how to reduce the risks. The aim is to lower the current recurrence rate, resulting in an improved quality of life for patients and a reduced financial burden to the NHS.
Conclusion
In order to receive payment for managing patients with VLUs, the focus is now more on the assessment, diagnosis and treatment, rather than prevention of recurrence. It could be argued, however, that it is more financially beneficial for leg ulcer services if ulceration recurs, which is a short-sighted view, particularly from the patient perspective. VLUs impact negatively on quality of life in terms of pain, mobility, and a restricted life with frequent appointments for treatment for patients. From the NHS perspective, VLUs are also expensive to treat in terms of nursing time, dressings etc, so it is clear that ulcer recurrence rates must be improved. This article has discussed how clinicians can encourage patients to perform self-care activities to prevent their ulcer recurring, which would improve their quality of life while reducing the financial burden of treating open ulceration for the NHS.
KEY POINTS:
- Chronic venous leg ulcers (VLUs) are commonly seen in general practice and although healing rates for leg ulcers have improved, recurrence rates are high with around 60–70% reported to recur after healing
- VLUs impact negatively on quality of life in terms of pain, mobility, and a restricted life with frequent appointments for treatment for patients
- The primary prevention strategy is the life-long wearing of compression hosiery; however, rates of patient intolerance are high
- Practice nurses can advise on self-care strategies such as physical exercise and mobility, leg elevation and appropriate skin care, to help prevent recurrence of venous leg ulcers
CPD reflective practice:
- How could you encourage compliance with compression hosiery?
- What self-care activities could you suggest to your patients to prevent recurrence of venous leg ulcers?
- How could you assess patient self-efficacy to take part in venous leg ulcer prevention strategies?